Introduction:
Dr. Bessel Van Der Kolk, a psychiatrist, researcher, and trauma specialist, writes in his book The Body Keeps The Score that “being traumatized means continuing to organize your life as if the trauma were still going on—unchanged and immutable—as every new encounter or event is contaminated by the past.” (Kolk, 2015). According to statistics from 1998, one in five Americans was sexually molested as a child, one in four were beaten by a parent enough to leave a mark on their body, and instances of physical violence occur in one out of three couples. One in four have alcoholic relatives and one in eight witnessed their mother being beaten or hit (Filetti et al., 1998). Trauma is not just the reality of soldiers and refugees. It permeates our homes, our neighborhoods, our cities, our countries, and the world. People develop Post Traumatic Stress Disorder (PTSD) when their normal coping mechanisms for stress are overwhelmed and they are frozen in the moment of trauma.
The predominant treatments for trauma and PTSD are medications and traditional talk therapies (Norman, Hamblen, Schnurr & Eftekhari, 2018). While they can facilitate understanding and numb overwhelming emotion, Van Der Kolk writes that “[w]hen the alarm bell of the emotional brain keeps signaling that you are in danger, no amount of insight will silence it.” (Kolk, 2015). This is especially true for trauma; talk therapy can be unhelpful and numbing emotion does not deal with the problem. Time Magazine reported on a study that evaluated the effectiveness of cognitive processing therapy (CPT) and prolonged exposure (PE), two of the front line talk therapy treatments for PTSD (Sifferlin, 2015). For both treatments, a full two thirds of participants still had symptoms severe enough to be diagnosed with PTSD at the end of the study. Effective treatments must find another way to help people heal. Van Der Kolk argues for a bottom-up, body-based, approach. In Van Der Kolk’s words, we need to give people “experiences that deeply and viscerally contradict the helplessness, rage or collapse that result from trauma” (Kolk, 2015).
In the last twenty years, psychiatric and psychological communities have developed and begun to integrate body-based approaches into therapy practices. Two such examples are Peter Levine’s Somatic Experiencing and Pat Ogden’s Sensorimotor Psychotherapy (Levine, n.d.; Ogden, n.d.). These programs are leading the way in integrated approaches to trauma therapy (Brom et al., 2017; Gene-Cos, Fisher, Ogden, & Cantrel, 2016). Unfortunately, there are far too few programs like these that focus on body-based trauma healing and can be integrated into therapy. Additionally, subtle differences in programs are important; what works for one person might not work for another. Therefore, as new programs are developed, it is important that they have diverse frameworks, so practitioners can create client-specific treatments.
When creating a new program about the body, it is important to consult people who understand the body. This study consults dance, a field whose very medium is the body. Specifically, the dance form Contact Improvisation, or Contact, is unique in its potential to help build a therapy program focused on bodily awareness. In 1972, Steve Paxton created a performance at Oberlin College called Magnesium. The performance was an experiment of weight and gravity, a group of men spent the performance falling over each other one moment, and standing upright attuning to the smallest shifts in balance the next. These two extremes both center around an ability to focus on bodily sensation; this performance is widely acknowledged as the birth of Contact.
Contact Improvisation today is based on the principle that if two or more people lean against each other and share their weight, they now have one shared center of gravity. The form itself is learning how to shift and manipulate that shared center. Contact values not how the dance looks, but how it feels. The focus is not on an outside audience member (as in more traditional dance forms) but on the relationship with your dance partner and your own body. In other words, Contact is based on bodily awareness. It also has a unique emphasis on trust and connection with others, both of which have their place in a therapeutic setting. The form has the potential to be developed into a highly effective trauma therapy program. Movement that involves a focus on bodily sensation has substantial health benefits on its own (Fogel, 2010). The findings of this research have implications beyond trauma to general health and wellbeing. This experiment will attempt to be the first piece of empirical evidence to demonstrate that, by focusing on whether Contact changes bodily awareness.
The stakes are extremely high for creating more trauma therapy programs. Millions of individuals are affected and untreated because of a lack of effective treatments of trauma. Trauma and PTSD lead to a host of other illnesses and conditions, but those are just symptoms. If we can not treat the actual problem, people get bounced from practitioner to practitioner with no improvement to their quality of life. Research has identified bodily awareness, or interoception as it is referred to in psychological studies, as an element that some effective trauma therapies have included. In his book In An Unspoken Voice, Peter Levine vividly writes about the biological underpinnings of trauma, and why interoception must play such a crucial role in its treatment (Levine, 2010). He starts by highlighting the speed with which humans register threat. If someone is walking through the woods and a deadly snake catches the eye, the body tenses and recoils a split second before your rational mind realizes it is just a stick. All animals are trained evolutionarily to attune to potential threats, and this analysis happens before the conscious mind is consulted. Levine points out another bodily mechanism of trauma, called tonic immobility. After fight or flight have been tried or suppressed, animals (humans are no exception) enter this state of immobile disassociation. Pain and movement are numbed, as is the experience of terror. Alone, tonic immobility does not create trauma, and in the wild it may even save an animals life. Many people may have seen a cat playing with a mouse that seems to be dead, but then it races off surprising the cat and surviving another day. Trauma occurs when tonic immobility is paired with intense terror and a person is restrained from life-saving action. This suppression can be physically as from an assaulter, but it can also be self-imposed as in the soldier who can’t flee without being dishonorably discharged as a coward. When these three factors come together, people can become stuck in the trauma, and this is where interoception comes in. In the example of the soldier, even after he is home from battle, the feelings of shame and terror stay with him. He is ashamed for freezing, and terrified of the battlefield, yet they are both behind him. Those feelings are then transferred to his own bodily sensations. He responds with the same kind of fear shutdown when those feelings surface. The solution for many is disassociation, repressing bodily sensations as much as possible. For people stuck in trauma like this, gradually training interoceptive awareness and un-conditioning their fear to those sensations is critical for treatment. Other research on body-based treatments for trauma, like yoga and Somatic Experiencing (Peter Levine’s treatment mentioned above), has also identified interoception as a critical focus for these programs to have (Payne, Levine, & Crane-Godreau, 2015; Price et al., 2017; Neukirch, Reid, & Shires, 2019).
This study focuses on interoception; it compared participants in dance classes over the course of a semester. A Contact Improvisation class was compared to a Contemporary 100 dance class, and a Psychology 100 class was used as a control. Each class’s interoceptive awareness was measured three times over the course of a semester. The Contact class is what this study is testing, the Contemporary class was chosen to make sure any effect Contact Improvisation had was not due just to the fact that it is a dance class, but that it is unique to Contact. The Psychology class was chosen as a control class that does not involve the body. The hypothesis for this experiment is that participants in the Contact Improvisation class will show the most increase in interoception through the course of the semester, and that the intro dance class will improve the second most. Since interoception has been identified as a key element in body based trauma therapies, if the hypothesis is correct, Contact Improvisation may have potential to be developed into an effective treatment. With every new program that deals directly with trauma and is shown to be effective, we lay down an infrastructure that will help our friends, families, communities and our society as a whole.
Methods:
The goal of this experiment is to demonstrate that Contact Improvisation increases bodily awareness.
Participants
In this study, three groups were compared. All three were college classes, so the study took place over the course of one semester. One group was a student taught Contact class, one was a college level “Intro to Contemporary Dance” class, and the third was a Psychology 100 class as the control. The Contact class met once a week for two hours over the semester, and the class has a mixture of exercises and improvised exploration. The Contemporary class met twice a week for an hour and a half each day, students learned specific dance techniques and choreography. The Psych class also met twice a week for an hour and fifteen minutes each day, they learned basic principles of psychology in a lecture setting. There were 5 participants from the Contact class, 6 from the Contemporary class and 9 from the Psych 100 class.
As incentive to participate in the study, the results from their specific interoception tests were offered to participants after all trials had been completed. The Psychology students were offered both that information as well as extra credit for their class, as organized through the Oberlin College Psychology Department.
Procedure
At the beginning, middle and end of the semester they were all measured on an objective and subjective interoception measure that had been shown to be reliable and valid. For the objective measure, participants did a heartbeat tracking task (Garfinkel, Seth, Barrett, Suzuki, & Critchley, 2015). The participants had their heartbeats monitored with a pulse oximeter finger cuff. The cuff ticks clearly at every heartbeat. With the cuff out of sight, they were told to count how many times their heart beat from when the researcher said “start” to when a timer went off, without feeling their pulse with their finger. Each participant at every time did six trials, at intervals of 25, 30, 35, 40, 45 and 50 seconds in random order. The researcher counted the actual number of times their heart beat in the timeframe.
The subjective measure was a self-report questionnaire that has been tested for reliability and validity. The Multidimensional Assessment of Interoceptive Awareness, or the MAIA, was used (Mehling et al., 2012). The MAIA is a 32 question survey, where participants answer questions on a 0-5 Likert Scale[3] . Before the 32 questions, three background questions were added. They were “Have you ever taken a dance class before?”, “Do you have any experience dancing Contact Improvisation before?” and “Have you ever taken a Contact Improvisation class before?”, and all three had yes or no options.
Results:
To test the hypothesis, a repeated measures ANCOVA was run for the heartbeat task by class, and a repeated measures ANOVA for the MAIA by class. Testing the session by class interaction for each will reveal if there were any differences in body awareness over the semester by class. The cell sizes, means and standard deviations for the two 3×3 factorial designs are reported in Table 1. The values for the heartbeat task are the means of difference scores. For each participant at each session, both their guess and their actual number of heart beats were collected for the six trials. The absolute value of their guess subtracted by the observed score for each trial were averaged together. This means that higher scores are less accurate, while lower scores are more accurate. The MAIA had thirty two questions, all scored on a scale between zero and five. Questions five through nine were reverse-coded, the others were scored as marked. All thirty two questions were averaged for each participant at each session. For this measure, higher scores signify more bodily awareness. A reliability analysis was also run for the survey, for each session, chronbach’s alpha = 0.799 for session one, 0.921 for session two and 0.943 for session three. All three of these scores are high, especially the second and third session. This means that the scale is reliable, for all three trials.
Several additional measures were created to be possible covariates. Three covariates were eventually used for the heartbeat analysis, while none were used for the MAIA. One of the covariates used was participant’s average heart rate between the three sessions. For the next, a measure of previous dance experience was used. On the first session participants were asked “Have you ever taken a dance class before”, “Do you have any experience dancing Contact Improvisation”, and “Have you ever taken a Contact Improvisation class before”. Their yes or no answers were summed to create a measure of background experience. The highest score could be a three, if participants answered yes to all three, the lowest score could be zero. The third covariate that was used in the analysis was one of the eight MAIA subscales identified by Mehling et al., 2012. The subscale used is called “Noticing”, and the questions in that subscale focus just on observation of bodily sensations. The first session data of this subscale were used. The other seven subscales in the MAIA, along with if participants are student athletes, were looked at as possible covariates but found not to explain a significant amount of variance in the heartbeat scores. None of the possible covariates mentioned explained a significant amount of variance in the MAIA scores.
In the repeated measures ANCOVA and ANOVA two effects are relevant to the hypothesis of the study. One is the session by class interaction, which will tell us if there is a difference in how the classes changed on the measures over the course of the semester. The other effect of importance is the between subjects analysis of class. This will tell us not about the change over time compared to the other sessions, but if the actual values are significantly different between the classes. For both the heartbeat scores and the MAIA scores, the between subjects variable class was highly significant. For the heartbeat, F(2, 14) = 13.053, p < .01, partial eta squared = 0.651; and for the MAIA, F(2, 17) = 12.599, p < .001, partial eta squared = 0.597. As shown in the descriptive statistics in Table 1, for the heartbeat scores the Psychology class scored better than both other classes each session. This seems to be random error, the groups started off unequal like this, and that difference held up throughout the semester. This was not quite so with the MAIA. The Contemporary class started with the highest scores, and kept those high scores throughout the study. The difference was not quite as pronounced in the MAIA as it was in the heartbeat scores.
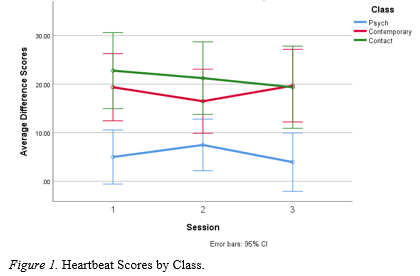
To test the hypothesis that the Contact class would improve more than the other two classes, the session by class interaction was examined. For the heartbeat scores, that interaction was not significant, F(4, 28) = 0.690, p = 0.605, partial eta squared = 0.090 (Table 2). However, because the cell sizes were so small for this study, it does not necessarily mean that there was no effect. The effect size is moderate even though the interaction was not significant. If we look at the graph of the three classes over time, we see that the Contact class was the only class to improve consistently each session, there was more variation in the other two (Figure 1). For the MAIA scores, the session by class interaction was significant, F(4, 34) = 2.943, p = 0.034, partial eta squared = 0.257 (Table 3). The results from the MAIA were clearer than the heartbeat. By looking at the graph (Figure 2) it is clear that both dance classes improved consistently over the semester while the Psychology class actually worsened.
There was one fairly extreme outlier in the Contact class for the study. They were an outlier only for the heartbeat test, not for the MAIA. As the researcher, I chose to keep them in the main analysis because while their difference scores were much higher than others’, they improved with each session in a similar manner to others in their class. When analyzing with them removed, the changes over the semester were almost exactly the same, but each value was lower. With the outlier included, the means and standard deviations of the Contact class for each session in order were 19.53 (18.22), 18.93 (18.44), and 17.77 (16.48). When the outlier was removed, they drop significantly to 12.13 (8.75), 11.67(10.07), and 11.29 (9.08). The scores still improve over the semester, but the values are much lower, lower than the Contemporary class.
Discussion:
The results of this study are tentative at best. The cell sizes are so small, it is hard to piece out what is error and what is an effect that would support or counter the hypothesis. The result that can be asserted most confidently is that the two dance classes improved significantly more than the psychology class on the MAIA survey. This supports part of the hypothesis, that dance could foster interceptive awareness, but doesn’t support the part that says Contact Improvisation is specifically suited for teaching this kind of awareness. The Contact class technically did improve more than the Contemporary class, but the difference is so slight that that difference is not statistically significant. It could be that the two dance forms teach bodily awareness similarly. There was also no significant difference between the classes in the heartbeat scores. It seemed that there may have been some error in those results, because they changed unpredictably and unexplainably from this hypothesis. The Contact class was the only one to improve over both sessions, though the difference between the classes was not significant. It is possible that the effect is there and the model didn’t pick it up because there were so few participants, but we would need to rerun the study with more participants to be able to show or assert that with any confidence. The fact that it had a moderate effect size makes this possibility more plausible than it would be otherwise.
Still, with such inconclusive results, it is hard to draw larger conclusions from this study. There are a few, however. The operationalization of the overall research question was very specific. The focus of this experiment was on interception. But Contact Improvisation has many other aspects of it that are well suited for a therapeutic environment. The dance form places a unique emphasis on trust, support, and connection. These are fundamental tenants of whole therapeutic orientations, like humanistic and mindfulness based orientations (Rogers, 1946; Neasciu & Linehan, 2014). There are also overlaps with specific Contact exercises to exercises already used in established therapies. For example, in Cognitive Behavioral Therapy (CBT) for panic disorder, it is thought that catastrophic reactions to interceptive sensations play a role in causing panic attacks. Therefore, one kind of exercise used in that treatment is called interoceptive exposure, where you expose a client to sensations that may make them anxious and then help them to sit through it and realize they are ok (Craske & Barlow, 2014). Some specific ways to do this are spinning in a chair, or shortened breathing. Contact Improvisation has many exercises similar, designed to induce and practice navigating disorienting sensations. Partner rolling and spinning lifts are examples from Contact that are close to these CBT exercises. Elements of Contact Improvisation are already practiced in therapeutic settings, in many different orientations. There is also research that links bodily awareness to trauma recovery. If future research can confirm more conclusively a link between practicing this form and interception, Contact will be well situated to be developed into an effective trauma therapy program.
References:
Brom, D., Stokar, Y., Lawi, C., Nuriel-Porat, V., Ziv, Y., Lerner, K., & Ross, G. (2017). Somatic Experiencing for Posttraumatic Stress Disorder: A Randomized Controlled Outcome Study. Journal of Traumatic Stress, 30(3), 304-312. doi:10.1002/jts.22189
Craske, M. G., & Barlow, D. H. (2014). Panic disorder and agoraphobia. In D. H. Barlow (Ed.), Clinical Handbook of Psychological Disorders: A Step-by-Step Treatment Manual. New York, NY: The Guilford Press.
Filetti V., et al. (1998). “Relationship of Childhood Abuse and Household Dysfunction To Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study” American Journal of Preventive Medicine 14, no. 4: 245-58
Fogel, A. (2010, July 6). Slow Movement with Awareness: Better than Exercise? Psychology Today.
Garfinkel, S. N., Seth, A. K., Barrett, A. B., Suzuki, K., & Critchley, H. D. (2015). Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biological Psychology, 104, 65-74. doi:10.1016/j.biopsycho.2014.11.004
Gene-Cos, N., Fisher, J., Ogden, P., & Cantrel, A. (2016). Sensorimotor Psychotherapy Group Therapy in the Treatment of Complex PTSD. Annals of Psychiatry and Mental Health. Retrieved from https://www.yellowbrickprogram.com/resources/pdf/Sensorimotry-Psychotherapy-Group-Therapy-Treatment-Complex-PTSD.pdf.
Kolk, B. V. (2015). The Body Keeps the Score. Penguin.
Levine, P. (n.d.). About Us. Retrieved from https://traumahealing.org/about-us/
Levine, P. A. (2010). In an Unspoken Voice: How the Body Releases Trauma and Restores Goodness. Berkeley, CA: North Atlantic Books.
Mehling WE, Price C, Daubenmier JJ, Acree M, Bartmess E, et al. (2012) The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLOS ONE 7(11): e48230. https://doi.org/10.1371/journal.pone.0048230
Neasciu, A. D., & Linehan, M. M. (2014). Borderline personality disorder. In D. H. Barlow (Ed.), Clinical Handbook of Psychological Disorders: A Step-by-Step Treatment Manual. New York, NY: The Guilford Press. 394-395 & 412-455.
Neukirch, N., Reid, S., & Shires, A. (2019). Yoga for PTSD and the role of interoceptive awareness: A preliminary mixed-methods case series study. European Journal of Trauma & Dissociation, 3(1), 7-15. doi:10.1016/j.ejtd.2018.10.003
Norman, S., Hamblen, J., Schnurr, P. P., & Eftekhari, A. (2018, September 28). Overview of Psychotherapy for PTSD. Retrieved from https://www.ptsd.va.gov/professional/treat/txessentials/overview_therapy.asp#backtotop.; Jeffreys, M. (2018, October 15). Clinician’s Guide to Medications for PTSD. Retrieved from https://www.ptsd.va.gov/professional/treat/txessentials/clinician_guide_meds.asp.
Ogden, P. (n.d.). About Sensorimotor Psychotherapy Institute. Retrieved from https://www.sensorimotorpsychotherapy.org/about.html
Payne P, Levine PA and Crane-Godreau MA (2015) Somatic experiencing: using interoception and proprioception as core elements of trauma therapy. Front. Psychol. 6:93. doi: 10.3389/fpsyg.2015.00093
Price, M., Spinazzola, J., Musicaro, R., Turner, J., Suvak, M., Emerson, D., & Kolk, B. V. (2017). Effectiveness of an Extended Yoga Treatment for Women with Chronic Posttraumatic Stress Disorder. The Journal of Alternative and Complementary Medicine, 23(4), 300-309. doi:10.1089/acm.2015.0266
Rogers, C. R. (1946). Significant aspects of client-centered therapy. American Psychologist, 1, 415-422.
Sifferlin, A. (2015, August 4). How Effective Are PTSD Treatments for Veterans? Time. Retrieved March 18, 2019, from http://time.com/3982440/ptsd-veterans/
Tables



Figures